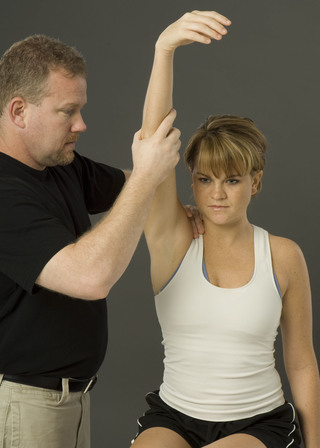
Brachial Plexus Stretch test |
Patient Position: Subject sits and the examiner stands behind the subject and places hand on one side of the subject's head and the other hand on the shoulder of that side.
Action: Examiner laterally flexes the subject's he'd while applying gentle downward pressure on shoulder.
+ Pain that radiates into the subject's arm opposite to the laterally flexed neck.
Action: Examiner laterally flexes the subject's he'd while applying gentle downward pressure on shoulder.
+ Pain that radiates into the subject's arm opposite to the laterally flexed neck.

Brachial Plexus Tension Test. (n.d.). [Untitled picture of stretch test] retrieved October 18th, 2015, from http://i.ytimg.com/vi/NswpZqnfmfQ/hqdefault.jpg
Piano Key sign
Patient Position: Subjects sits with the involved limb relaxed at the side, or stands facing the examiner.
Action: Apply pressure to the subject's distal clavicle in an inferior direction.
+ Instability of the AC joint on the involved side.
Action: Apply pressure to the subject's distal clavicle in an inferior direction.
+ Instability of the AC joint on the involved side.

SC Joint Stress test
Patient Position: Subject stands with involved arm relaxed at the side. The examiner stands in front of the subject placing one hand on the proximal end of the subject's clavicle and the other hand on the spine of the scapula.
Action: Apply gentle inferior and posterior pressure on the clavicle.
+ Pain and/or movement of the clavicle indicates a sternoclavicular ligament sprain
Action: Apply gentle inferior and posterior pressure on the clavicle.
+ Pain and/or movement of the clavicle indicates a sternoclavicular ligament sprain

Motion Test of the SC-Joint (n.d.). [Untitled picture of SC stress] retrieved October 18th, 2015, from http://i.ytimg.com/vi/gKERPpqMXtI/maxresdefault.jpg
Hawkins-Kennedy Impingement test
Patient Position: Sitting or standing with both upper extremities relaxed. The examiner stands with one hand grasping the subject's elbow and the other hand grasping the subject's wrist.
Action: Examiner forward flexes the shoulder to 90 degrees and then internally rotates the subject's test shoulder.
+ Shoulder pain and apprehension are indicative of shoulder impingement, particularly of the supraspinatus tendon.
Action: Examiner forward flexes the shoulder to 90 degrees and then internally rotates the subject's test shoulder.
+ Shoulder pain and apprehension are indicative of shoulder impingement, particularly of the supraspinatus tendon.

Board and Spine (n.d.). Hawkins-kennedy-impingement-test retrieved October 18th, 2015, from http://i0.wp.com/boneandspine.com/wp-content/uploads/2011/10/hawkins-kennedy-impingement-test.jpg
Neer Impingement test
Patient Position: Sitting or standing with both upper extremities relaxed. The examiner stands with one hand on the scapula and the other hand grasping the subject's elbow.
Action: Examiner passively and maximally forward flexes the shoulder.
+ Shoulder pain and apprehension are indicative of shoulder impingement, particularly of the supraspinatus and bicep long head tendon,
Action: Examiner passively and maximally forward flexes the shoulder.
+ Shoulder pain and apprehension are indicative of shoulder impingement, particularly of the supraspinatus and bicep long head tendon,
Gallerygopix (2015). Neer sign shoulder the Neer impingement Sign retrieved October, 18th, 2015, from http://jurchperformanceeducation.com/wp-content/uploads/2013/02/Neer1.jpg
Cross-Over Impingement test
Patient Position: Subject Sits. Examiner stands with one hand on the posterior aspect of the subject's shoulder to stabilize the trunk and the other hand grasping the subject's elbow on the the test arm.
Action: With the subject's trunk stabilized, the examiner passively and maximally horizontally adults the test shoulder.
+ Superior shoulder pain is indicative of AC joint pathology. Anterior shoulder pain is indicative of subscapualris, supraspinatus and/or biceps long head pathology. Posterior shoulder pain is indicative infraspinatus, trees minor, and/or posterior capsule pathology.
Action: With the subject's trunk stabilized, the examiner passively and maximally horizontally adults the test shoulder.
+ Superior shoulder pain is indicative of AC joint pathology. Anterior shoulder pain is indicative of subscapualris, supraspinatus and/or biceps long head pathology. Posterior shoulder pain is indicative infraspinatus, trees minor, and/or posterior capsule pathology.

Cross-Over Impingement (n.d.) [Untitled Cross Over] retrieved October 18th, 2015, from http://i.ytimg.com/vi/hgWcooTACK8/mqdefault.jpg
Apley's Scratch test
Patient Position: Subject may sit or stand, the examiner stands next to subject.
Action: Subject is instructed to take one hand and touch the opposite shoulder.
+ Asymmetrical results from side to side. 1) Inability to touch opposite shoulder is indicative of limited glenohumeral adduction, internal rotation and horizontal flexion. 2) Decreased motion is indicative of limited glenohumeral abduction, external rotation and scapular upward rotation and elevation. 3) Decreased motion is indicative of limited glenohumeral adduction, internal rotation and scapular retraction and downward rotation.
Action: Subject is instructed to take one hand and touch the opposite shoulder.
+ Asymmetrical results from side to side. 1) Inability to touch opposite shoulder is indicative of limited glenohumeral adduction, internal rotation and horizontal flexion. 2) Decreased motion is indicative of limited glenohumeral abduction, external rotation and scapular upward rotation and elevation. 3) Decreased motion is indicative of limited glenohumeral adduction, internal rotation and scapular retraction and downward rotation.

Grab Page (n.d) [Untitled Apley scratch] retrieved October 18th, 2015, from http://b.vimeocdn.com/ts/441/774/441774038_640.jpg
Drop Arm test
Patient Position: Sits or Stands
Action: Examiner Passively abducts the subject's involved arm to 90 degrees and then instructs them to slowly lower the arm to their sides.
+ The subject is unable to slowly return the arm to the side and/or has significant pain. Test for rotator cuff pathology
Action: Examiner Passively abducts the subject's involved arm to 90 degrees and then instructs them to slowly lower the arm to their sides.
+ The subject is unable to slowly return the arm to the side and/or has significant pain. Test for rotator cuff pathology

Drop Arm Special Test (n.d.) [Untitled Drop Arm] retrieved October 18th, 2015, from https://i.ytimg.com/vi/CEKWtmyPsTA/maxresdefault.jpg
Ludington's sign
Patient Position: Examiner stands directly behind the subject. The subject interlocks his fingers and places them on the superior/posterior aspect of the head.
Action: Examiner palpates the long head of the biceps tendon bilaterally while the subject contracts both biceps brachii.
+ Increased pain is indicative of a bicep brachia long head tendinitis. Decreased tension of the tendon with palpation may indicate an inability of the biceps tendon to contract
Action: Examiner palpates the long head of the biceps tendon bilaterally while the subject contracts both biceps brachii.
+ Increased pain is indicative of a bicep brachia long head tendinitis. Decreased tension of the tendon with palpation may indicate an inability of the biceps tendon to contract

Shoulder Orthopedics (2015) Lundington retrieved October 18th, 2015, from https://classconnection.s3.amazonaws.com/219/flashcards/3097219/png/ludingtonjpg1366484888205.png
Speed's test
Patient Position: The involved shoulder is flexed to 90 degrees, the elbow is fully extended, and the forearm is supinated. Examiner places on hand along the the subject's forearm and the other hand on the the bicipital groove.
Action: Resist the attempt to actively flex the humerus forward.
+ Tenderness and/or pain in the bicipital groove. Test for bicep tendinitis
Action: Resist the attempt to actively flex the humerus forward.
+ Tenderness and/or pain in the bicipital groove. Test for bicep tendinitis

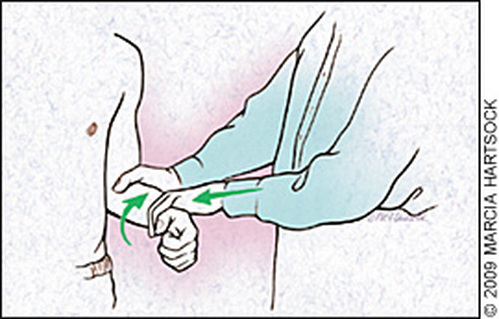
Yergason test
Patient Position: Elbow flexed to 90 degrees and stabilized against the thorax. Forearm pronated and the examiner places one hand along the subject's forearm and the other hand on the proximal portion of the subject's humerus over the bicipital groove.
Action: Resist the attempt to actively supinate the forearm and externally rotate the humerus.
+ Pain that is reported to exist in the area of the bicipital groove. Test for bicep tendinitis
Action: Resist the attempt to actively supinate the forearm and externally rotate the humerus.
+ Pain that is reported to exist in the area of the bicipital groove. Test for bicep tendinitis
AAFP (2009) Figure 2. Yeargason Test retrieved October 18th, 2015, from http://www.aafp.org/afp/2009/0901/afp20090901p470-f2.jpg
O'Briens test
Patient Position: Subject sits or stands with the test shoulder in 90 degrees of forward flexion, 30-45 degrees of horizontal adduction and maximal rotation.
Action: The subject horizontally adducts and flexes the test shoulder against the examiners resistance.
+ Pain and/or popping that is present in the internally rotated position but absent in the externally rotated position is indicative of a SLAP lesion.
Action: The subject horizontally adducts and flexes the test shoulder against the examiners resistance.
+ Pain and/or popping that is present in the internally rotated position but absent in the externally rotated position is indicative of a SLAP lesion.

Orthopedic Surgery HC Chang (2010) SLAP Tear retrieved October 18th, 2015, from http://orthopaedic.com.sg/wp-content/uploads/2011/05/O-Briens-Test.jpg
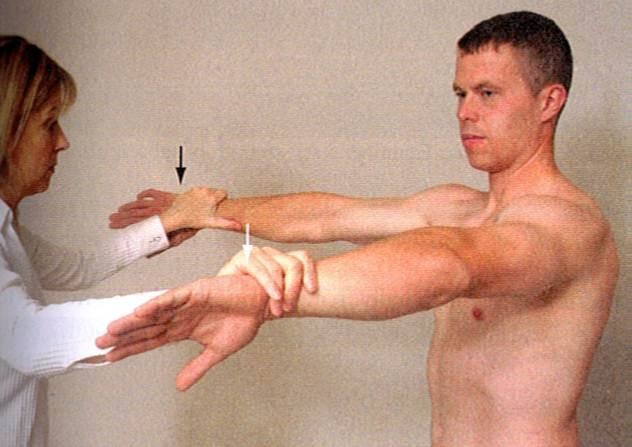
Empty can
Patient Position: Stands with both shoulders abducted to 90 degrees, horizontally adducted 30 degrees and internally rotated so thumbs face the floor.
Action: Resist the attempt to actively forward elevate both shoulders.
+ Involvement of the supraspinatus muscle/tendon is suspected with noted weakness and/or a report of pain.
Action: Resist the attempt to actively forward elevate both shoulders.
+ Involvement of the supraspinatus muscle/tendon is suspected with noted weakness and/or a report of pain.
Study Blue (n.d) [Untitled Empty Can] retrieved October 18th, 2015, from https://classconnection.s3.amazonaws.com/522/flashcards/1066522/jpg/empty_can1330050970924.jpg
AC compression
Patient Position: Subject sits with the involved arm relaxed at the side. The examiner stands on the involved side, placing one hand on the subject's clavicle and the other hand on the spin of the scapula.
Action: The examiner gently squeezes the hands together.
+ Pain and/or movement of the clavicle is positive for an acromioclavicular and/or coracoclavicular ligament sprain.
Action: The examiner gently squeezes the hands together.
+ Pain and/or movement of the clavicle is positive for an acromioclavicular and/or coracoclavicular ligament sprain.

Study blue (n.d) [Untitled AC compression] retrieved October 18th, 2015, from https://classconnection.s3.amazonaws.com/691/flashcards/2567691/jpg/ac_shear_test-1472BFE14CA0B222F2C.jpg
Sulcus sign
Patient Position: Subject sits wit forearms and hands resting. Examiner stands with proximal hand grasping the subject's scapula and the distal hand grasping the subject's elbow.
Action: Examiner applies an inferior force.
+ Excessive inferior humeral head translation with a visible and/or palpable "Step off". Indicative of inferior and/or multidirectional instability.
Action: Examiner applies an inferior force.
+ Excessive inferior humeral head translation with a visible and/or palpable "Step off". Indicative of inferior and/or multidirectional instability.

Sulcus Sign (n.d.) [Untitled Sulcus Sign] retrieved October 18th, 2015, from http://i.ytimg.com/vi/-IcFzkm_oQw/hqdefault.jpg
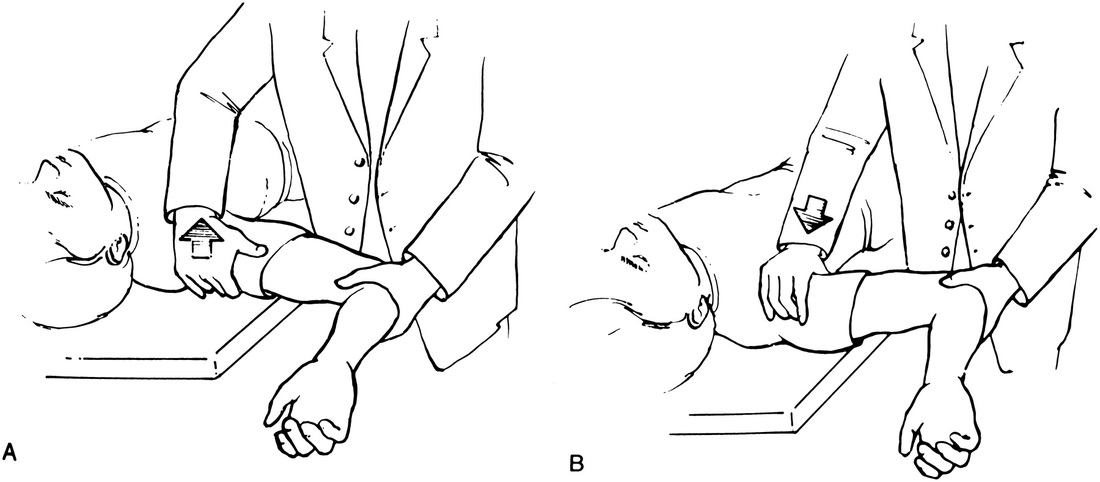
Anterior drawer
Patient Position: Subject lies supine with glenohumeral joint positioned at the edge of the table. Examiner places one hand around the surgical neck. The other hand stabilizing the scapula.
Action: Subject must remain relaxed while the examiner passively abducts the glenohumeral joint 70-80 degrees, forward flexes 0-10 degrees, externally rotates 0-10 degrees. Examiner firmly glides the head of the humerus anteriorly while applying slight distraction to the joint.
+ Increased anterior translation of the humeral head relative to the scapula/glenoid fossa may indicate anterior instability.
Action: Subject must remain relaxed while the examiner passively abducts the glenohumeral joint 70-80 degrees, forward flexes 0-10 degrees, externally rotates 0-10 degrees. Examiner firmly glides the head of the humerus anteriorly while applying slight distraction to the joint.
+ Increased anterior translation of the humeral head relative to the scapula/glenoid fossa may indicate anterior instability.

A+ Orthopedic and Sports Medicine Clinic (n.d.) [Anterior Drawer] Retrieved October 18th, 2015, from http://www.sportsmedicineclinicdelhi.com/shoulder_instability_files/image020.jpg
Posterior drawer
Patient Position: Subject lies supine with glenohumeral joint positioned at the edge of the table. Examiner places one hand around the surgical neck. The other hand stabilizing the scapula.
Action: Examiner applies downward pressure, pushing the head posteriorly.
+ Increased posterior instability of the humeral head relative to the scapula/glenoid fossa may indicate posterior instability.
Action: Examiner applies downward pressure, pushing the head posteriorly.
+ Increased posterior instability of the humeral head relative to the scapula/glenoid fossa may indicate posterior instability.

Sports Health (2014) [Evaluation and Management of Posterior Shoulder Instability] retrieved October 18th, 2015, from http://sph.sagepub.com/content/3/3/253/F1.large.jpg
Anterior apprehension
Patient Position: Subject lies spine on the table
Action: Subject's involved shoulder in 90 degrees of abduction and the elbow in 90 degrees of flexion, examiner slowly externally rotates shoulder
+ If the subject expresses apprehension towards further external rotation.
Action: Subject's involved shoulder in 90 degrees of abduction and the elbow in 90 degrees of flexion, examiner slowly externally rotates shoulder
+ If the subject expresses apprehension towards further external rotation.

Shoulder Anterior Apprehension (n.d.) [Untitled Apprehension} Retrieved October 18th, 2015, from https://i.vimeocdn.com/video/349342644_640.jpg
Jobe relocation
Patient Position: Subject lies supine with the test shoulder in 90 degrees of abduction and full external rotation. The examiner stands with the distal hand grasping the subject's wrist. The proximal hand is placed over the subject's humeral head.
Action: Apply a posterior force to the humeral head, while the examiner externally rotates the subject's humerus.
+ A reduction of pain and apprehension, and commonly an increase in shoulder external rotation, indicative of anterior instability.
Action: Apply a posterior force to the humeral head, while the examiner externally rotates the subject's humerus.
+ A reduction of pain and apprehension, and commonly an increase in shoulder external rotation, indicative of anterior instability.
The American Journal of Sports Medicine (2014) [Figure 8. Jobe relocation] retrieved October 18th, 2015, from http://ajs.sagepub.com/content/28/2/265/F8.large.jpg
Clunk and grind test
Patient Position: Subject lies supine on a table with the shoulder abducted to 90 degrees and the elbow flexed to 90 degrees. Examiner grasps the subject's elbow with one hand and the subject's proximal humerus with the other hand.
Action: Apply compression to the glenoid labrum while attempting to rotate the humeral head 360 degrees around the glenoid fossa.
+ Indicative of a glenoid labrum tear to the specific location.
Action: Apply compression to the glenoid labrum while attempting to rotate the humeral head 360 degrees around the glenoid fossa.
+ Indicative of a glenoid labrum tear to the specific location.

Mike Reinold (n.d) [Untitled Clunk and Grind] retrieved October 18th, 2015, from http://www.mikereinold.com/wp-content/uploads/blogger/43-DSC01936[4].jpg
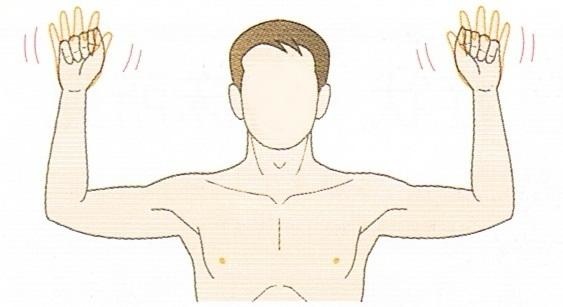
Roo's test
Patient Position: Subject sits or stands with both shoulders in 90 degrees of abduction and external rotation, and the elbows in 90 degrees of flexion.
Action: The Subject rapidly opens and closes both hands for 3 minutes.
+ The inability to maintain the test position, diminished motor function of the hands, and/or loss of sensation in the upper extremities are indicative of thoracic outlet syndrome secondary to neurovascular compromise.
Action: The Subject rapidly opens and closes both hands for 3 minutes.
+ The inability to maintain the test position, diminished motor function of the hands, and/or loss of sensation in the upper extremities are indicative of thoracic outlet syndrome secondary to neurovascular compromise.
Study Blue (n.d.) [Untitled Roo’s] retrieved October 18th, 2015, from https://classconnection.s3.amazonaws.com/580/flashcards/4609580/jpg/roos_test-14712348605655809D1.jpg
Allen's test
Patient Position: Subject sits or stands with test shoulder in 90 degrees of abduction and external rotation, and the elbow in 90 degrees of flexion. Examiner has fingers over radial artery.
Action: Subject rotates the neck away from the test arm while the examiner palpates the radial pulse.
+ A diminished or absent radial pulse is indicative of thoracic outlet syndrome.
Action: Subject rotates the neck away from the test arm while the examiner palpates the radial pulse.
+ A diminished or absent radial pulse is indicative of thoracic outlet syndrome.

NISMAT (2012) [Allen Test] retrieved October 18th, 2015, from http://www.nismat.org/data/images/allen10766392614.jpg
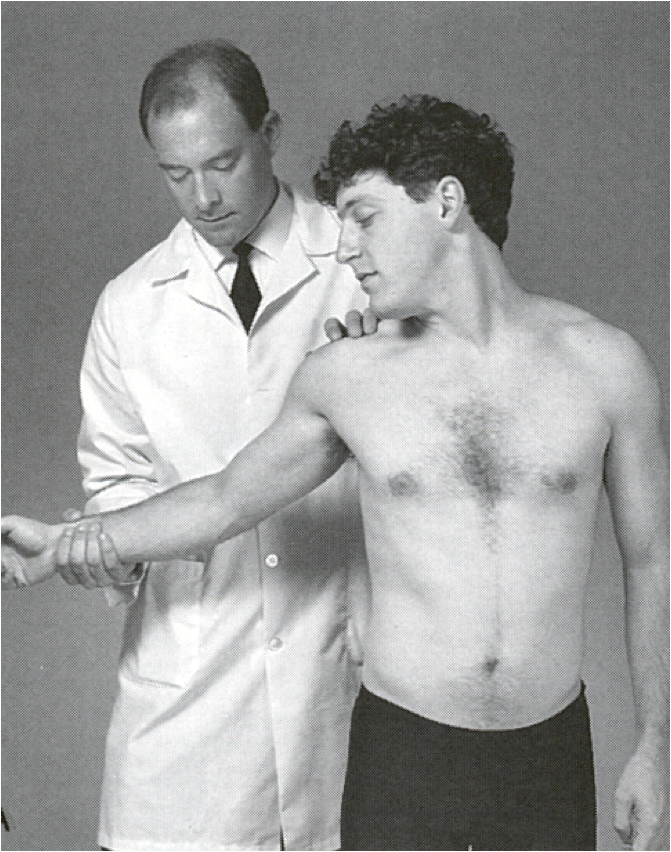
Adson's Maneuver Test
Patient Position: Subject sits or stands. Examiner stands with fingers over the radial artery.
Action: Externally rotate and extend the subject's arm while palpating the radial pulse. Subject then extends and rotates the neck toward the test arm and takes a deep breath.
+ A diminished or absent radial pulse is indicative of thoracic outlet syndrome, secondary to compression of the subclalvian artery by the scalene muscles.
Action: Externally rotate and extend the subject's arm while palpating the radial pulse. Subject then extends and rotates the neck toward the test arm and takes a deep breath.
+ A diminished or absent radial pulse is indicative of thoracic outlet syndrome, secondary to compression of the subclalvian artery by the scalene muscles.
Study Blue (n.d.) [Untitled Adson’s] retrieved October 18th, 2015, from https://classconnection.s3.amazonaws.com/1412/flashcards/809708/png/ads.png
All special test material was taken from (Konin, Wiksten, Isear Jr., J. A., & Brader (2006)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![http://www.mikereinold.com/wp-content/uploads/blogger/43-DSC01936[4].jpg](http://www.mikereinold.com/wp-content/uploads/blogger/43-DSC01936%5b4%5d.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}